
As the push for more school-based mental health intervention increases after recent high profile school shootings, one particularly controversial and inaccurate mental health screening instrument, “TeenScreen”, is starting to make a comeback. Developed by Dr. David Schaffer and other psychiatrists at Columbia University, TeenScreen is a 14-question computerized survey that was heavily used in as many as 40 states in the early 2000s.
However, the vague and subjective questions used by Teen Screen yielded an astronomical false-positive rate of 84 percent, as admitted by Dr. Schaffer:
The CSS’s positive predictive value of 16% (determined by a weighted prevalence of DISC positive in the sample) would result in 84 nonsuicidal [sic] teens being referred for further evaluation for every 16 youths correctly identified.
One egregious example of TeenScreen’s inaccuracy occurred when an Indiana high school student was forced to take the survey without her parents’ knowledge or consent. As a result of her Teen Screen responses, she was given two psychiatric diagnoses in the hall of the school by a perfect stranger. Because she was studious and did not like to party, she was labeled with social anxiety disorder, and because she liked to keep things clean, she was tagged with obsessive-compulsive disorder. The understandably outraged parents subsequently sued the school and mental-health agency administering TeenScreen.
The lawsuit and surrounding controversy caused the consent procedures to switch from opt-out to opt-in parental consent, resulting in a massive decline in the numbers of children screened (the Indiana school screening the student without parental consent stopping the procedure altogether). This change in consent procedure, the high false-positive rate, and the strong connection between TeenScreen and the pharmaceutical industry were all likely factors in forcing TeenScreen to eventually cease operations of its national program in 2012.
The Dangers of TeenScreen
However, this is unfortunately not the end of the TeenScreen saga. In 2016, Stanford University acquired the rights to the TeenScreen test, and it has been used in some school districts even as recently as the fall of 2018. Even more concerning is recent testimony by Dr. Mark Olfson, current scientific director of whatever is left of TeenScreen at Columbia University, before the federal School Safety Commission in July calling for expansion of “voluntary mental health screening” in an effort to prevent mass shootings such as the one at Parkland, Fla., despite other parts of his testimony rendering that recommendation dangerous and quite illogical:
There are concerns that many young people are being unnecessarily treated with these medications because approximately two-thirds of the increase, the overall increase in psychotropic medication use in youth has occurred among those with less severe or no impairment.
These concerns have focused most intensively on anti-psychotic medications, particularly their use in very young children and children in the foster care system.
He does not realize — or will not admit — that the reason the overall prescription rate increase has occurred in youth with “less severe or no impairment” is due to the promotion and widespread use of mental screening instruments like TeenScreen. Olfson does, however, admit some of the dangerous side effects of the medications:
In addition to uncertainty over the long-term effects on the developing brain, side effects of anti-psychotic medications include weight gain, high cholesterol levels and increased risk of diabetes.
Other severe and life-threatening effects associated with the antipsychotics (studies compiled here) include brain damage, movement disorders, suicide, and a 25-year shortened life span.
In addition, psychiatric experts readily admit that their efforts to predict which patients will become violent are only slightly better than chance, so it is unwise to train already overburdened school staff for a few hours and place this enormous responsibility on them. A psychologist involved in violence-prediction research told the Washington Post, “There is no instrument that is specifically useful or validated for identifying potential school shooters or mass murderers.” Another said in that same article that doing so would endanger both public safety and civil liberties.
Moreover, many experts also rejected the idea of expanded school mental-health screening after the horrific Sandy Hook shooting. A psychiatrist who extensively studied the Sandy Hook shooter told the Los Angeles Times after the Parkland massacre, “But unfortunately, it’s impossible for any of us to predict who is going to go from being troubled and isolated to actually harming others…It really means we can’t rely on prediction and identifying the bad guys. Because we’ll misidentify some who aren’t bad guys, and we’ll fail to identify others who may become bad guys.”
Financial Profit vs. Children’s Health?
Nevertheless, TeenScreen was heavily promoted via the New Freedom Commission on Mental Health during the George W. Bush administration. It was also heavily promoted by pharmaceutical industry front groups like the National Alliance for Mental Illness (NAMI), which acknowledged receiving 56 percent of its funding from the pharmaceutical industry after a congressional investigation conducted at that time showed that it received 81 percent of its funding from psychotropic drug manufacturers.
The New Freedom Commission also promoted something called the Texas Medication Algorithm Project (TMAP) that strongly recommended the use of new antipsychotic drugs that have extremely dangerous side effects (to be discussed below) and have been no more effective than the older drugs they sought to replace.
Both TeenScreen and TMAP were found to have strong ties to the pharmaceutical industry, according to whistleblower Allen Jones. Here is an excerpt from the Rutherford Institute’s interview (also here) of Jones explaining how the scheme worked:
An investigator for the Pennsylvania Office of the Inspector General (OIG), Jones’ findings in the case showed that the drug company Janssen had paid honorariums to key state officials who held significant influence over the prescriptions issued for state institutions such as prisons and mental health hospitals. Although the accounts receiving these payments were marked for “educational grants,” funds were being channeled to state employees who developed guidelines recommending new, more expensive drugs rather than older, cheaper drugs with safe, proven effects. These companies were influencing officials with trips, perks and lavish travel accommodations as a means of inducing the officials to endorse their products.
A small industry “investment” in TMAP resulted in blockbuster profits for the drug companies. Here is a table produced by a Texas TV station investigative report (as described here) demonstrating this phenomenon:
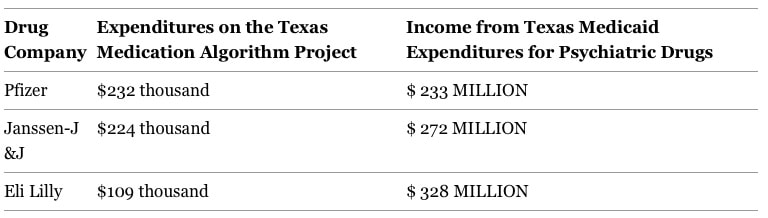
TMAP was exported to many states across the nation, and the drugs were heavily prescribed to those receiving Medicaid benefits, including those in the foster care system, as Dr. Olfson described in his testimony (more details here). To have these most vulnerable children prescribed such potent and dangerous drugs in the pursuit of profits instead of for real medical need is a tragedy.
For these reasons and many more, parents should be concerned with, and school administrators should be extremely wary of, the expansion of mental health screening. Please send your comments about this to the federal School Safety Commission at safety@ed.gov and to your state legislators if your state is pursuing these programs.

